
Public Health Agency of Canada
www.publichealth.gc.ca
Lyme disease and other tick-borne diseases: Information for healthcare professionals
Lyme disease is a multisystem illness caused by Borrelia burgdorferi, a spirochete transmitted by certain species of Ixodes ticks. The Public Health Agency of Canada (the Agency), in partnership with provincial and territorial public health authorities, conducts surveillance for Lyme disease in Canada and studies show that the incidence of this disease is on the rise in Canada.
The Agency encourages health professionals to learn about Lyme disease in Canada; how to identify the symptoms and prescribe proper treatment if a patient is diagnosed with the disease; and how to report cases of Lyme through appropriate channels.
The following information replicates what is currently captured in medical literature. The Agency acknowledges that there is more to learn about the epidemiology of Lyme disease and other tick-borne diseases in Canada. As well, clinical questions remain, such as why some individuals have persistent symptoms after treatment of their infection and how can we optimally diagnose re-infection. The Agency is committed to exploring new science and research to better detect, diagnose and treat Lyme disease.
On this page:
- Lyme disease in humans:
- Surveillance of Lyme disease cases
- Other tick-borne diseases in Canada
- Identifying blacklegged ticks
- Removing Ticks
- Submitting ticks for identification and testing
- References
Lyme disease in humans
At a glance
Lyme disease is a multisystem illness caused by B. burgdorferi, a spirochete transmitted by certain species of Ixodes ticks, specifically the blacklegged tick and the western blacklegged tick (Ogden et al. 2009). Ticks become infected by feeding on infected wild animal hosts, such as rodents and birds, and can then transmit the bacterium to humans. Infection with B. burgdorferi causes what is known as Lyme disease in humans.
Lyme disease is the most commonly reported vector-borne disease in the northern temperate zone. It became a nationally notifiable disease in December 2009. As such, all healthcare professionals are to report cases of Lyme disease to the Agency via their provincial or territorial public health system. The Agency posts information on notifiable diseases on its website.
The Agency currently has data for Lyme disease cases reported between 2009-2013*:
- 2009: 144 cases
- 2010: 143 cases
- 2011: 266 cases
- 2012: 338 cases
- 2013: 682 cases
- 2014: The Agency is still validating reports from provinces and territories. The final figure will be confirmed and reflected here.
Currently over 80% of reported cases were acquired in Canada.
The incidence of Lyme disease peaks in children between 5-9 years and adults between 55-59 years (Source: Bacon et al, 2008).
- Footnote *
- These numbers may change slightly as provincial and territorial public health departments can, from time to time, retroactively identify cases and update their statistics. Public health reporting gives us only part of the picture; the true number of Lyme disease cases in Canada is likely greater.
Post-treatment re-infection is possible, especially when a person is re-infected with different strains of B. burgdorferi.
Clinical presentation and course
The clinical manifestations of Lyme disease largely reflect the biology of B. burgdorferi as it replicates in the skin (early, localized Lyme disease, which sometimes presents as erythema migrans) and then disseminates (early and late disseminated Lyme disease) via the bloodstream to other body sites where the bacterium provokes damage to body tissues (Bockenstedt, p. 283, 2008). Symptoms appear, sometimes in overlapping stages, as early localized disease, early disseminated infection, or late disease.
Know the clinical manifestations and epidemiological risk factors, and consider Lyme disease as part of your differential diagnosis in a patient who presents with compatible symptoms and signs. Accurate diagnosis is one of the key factors to the successful management of Lyme disease.
Early Localized Disease
It is important to note that some people with Lyme disease may have no or minimal symptoms, yet others may suffer severe symptoms. As well, some people may not develop symptoms until weeks after the initial bite and. In this case, they may not remember the tick bite or associate the illness with the bite. Because the blacklegged tick is so small, some people may not even know that they had a tick bite.
A typical sign of early non-disseminated Lyme disease is an expanding rash called erythema migrans. Such a rash can occur at the site of the infective tick bite, usually within 7-14 days (range, 3-30 days) post infection and can persist up to 8 weeks. However, it is important to note that a rash is not manifested in all cases, and to watch out for other symptoms of the disease, including low-grade fever, fatigue, headache, and joint pain in order to inform a differential diagnosis.
A Note about Erythema Migrans
Evidence continues to emerge regarding the prevalence of the EM rash (an expanding macular erthematous rash, expanding outward from the location of the tick bite) and the frequency with which the EM takes on a bull’s eye appearance (red patch expanding outward with clearing occurring from the centre out).
While many medical textbooks indicate the EM occurs in 70-80% of cases, with the bull’s eye occurring in 50% of those cases; some recent studies suggest that the bull’s eye appearance occurs less frequently (Stonehouse et al. 2007).
It is important therefore that clinicians do not rely solely on the presence or absence of a bull’s eye rash for their diagnosis. While such a rash is highly suggestive of Lyme disease, it is not absolutely pathognomonic of Lyme disease, EM may take alternate forms — solid lesions, blue-purple hues, and crusted or blistering lesions have also been documented. The rash is not painful or pruritic, but it may be warm to the touch. In dark skinned patients, the EM may appear more as a bruise. Therefore, an absence of the bull’s eye rash or typical red EM does not preclude Lyme disease as the appropriate diagnosis.
Erythema migrans can take many forms such as:

Image 1: A typical sign of early non-disseminated Lyme disease is an expanding rash called erythema migrans, which can take on the appearance of a bull's eye.
Reproduced with permission from Dr. John Aucott, Lyme MD, Lyme Disease Research Foundation

Reproduced with permission from Dr. John Aucott, Lyme MD, Lyme Disease Research Foundation

Reproduced with permission from Dr. John Aucott, Lyme MD, Lyme Disease Research Foundation

Image 2: Some Lyme disease skin lesions are uniformly red and do not appear with the classic ring.
Reproduced with permission from Dr. John Aucott, Lyme MD, Lyme Disease Research Foundation

Reproduced with permission from Dr. John Aucott, Lyme MD, Lyme Disease Research Foundation

Early disseminated disease
If untreated, this stage of the disease can last up to several months and could include the following symptoms:
- Fatigue and general weakness
- Neurological: cranial neuropathy; meningitis; motor and sensory radiculoneuropathy, mononeuritis multiplex; subtle cognitive difficulties; encephalopathy; radiculopathy
- Cardiac - conduction abnormalities, e.g. atrioventricular node block; ventricular node block; myocarditis, pericarditis, sudden death
- Cutaneous (multiple EM lesions)
- Additional manifestations (conjunctivitis, keratitis, uveitis; mild hepatitis; splenomegaly)
Late Lyme disease
If it remains untreated, late Lyme disease can last months to years with symptoms that can include:
- Rheumatological –Asymetric oligoarticular arthritis especially involving the knees (chronic arthritis, transient, migratory arthritis and effusion in one or multiple joints; Baker’s cyst; if untreated, arthritis may recur in same or different joints).
- Neurological (Subacute mild encephalopathy affecting memory and concentration, chronic mild axonal polyneuropathy manifested as distal paresthesias and less commonly, as radicular pain). Rarely, an encephaolomyelitis or leukoencephalopathy may occur.
Diagnosis
In general, the diagnosis of Lyme disease is principally clinical, supported by a history of potential tick exposure in an area where it is known or suspected that blacklegged ticks have become established. It is important to obtain an accurate exposure history, including both local and distant travel to endemic or emerging risk areas. However, as tick populations are expanding, it is possible that Lyme disease can be acquired outside the currently identified areas and this should be considered when assessing patients. Detection of antibodies against B. burgdorferi using the two-tiered serological method described below is an additional diagnostic tool; however patients with clear symptoms of early localized Lyme disease should be diagnosed and treated without laboratory confirmation, as false negative test results are common during the early stage of Lyme disease.
Laboratory diagnosis
Laboratory confirmation of B. burgdorferi infection is problematic. Antibody testing can contribute to the diagnosis but only under carefully selected conditions and at the risk of generating false-positive results. Isolation of the spirochete is not practical, and the DNA detection by PCR technology is experimental. As such, the diagnosis of Lyme disease is predominantly a clinical one. Laboratory testing should only be used as a supplement to the clinical findings and not as a basis for diagnosis. (Goroll, 2014, p. 1156) That said, the current diagnostic tests used in Canada are appropriate tools for diagnosis of early and late disseminated Lyme disease.
The most common diagnostic approach used to supplement clinical suspicion of Lyme disease is the demonstration of B. burgdorferi-specific antibodies in the patient’s serum. A two-tiered algorithm (see next section) is recommended – an EIA (enzyme immunoassay) should be performed first; and if positive or equivocal, it is followed by a Western blot assay. Western blot results should be interpreted according to Infectious Disease Society of America (IDSA) guidelines to obtain the best balance between sensitivity and specificity.
In suspected Lyme meningitis, testing by an accredited laboratory, for intrathecal IgM or IgG antibodies may be helpful. All of the diagnostic laboratories across Canada have accredited, quality systems in place (such as CAP, OLA or ISO) either for all procedures or testing conducted in the laboratory or specifically for Lyme disease serological testing. Furthermore, all serological tests for Lyme disease used in these labs have been licensed for this use by Health Canada and they participate in external proficiency testing to ensure high quality results.
Laboratory testing
Serological and DNA tests can be helpful under certain circumstances, particularly in supporting the clinical impression of early and late disseminated Lyme disease.
Two-tiered testing method
The Agency’s National Microbiology Laboratory (NML) and some provincial laboratories assist clinicians to diagnose Lyme disease using a two-tiered serological testing approach that includes an EIA screening test followed by a confirmatory Western blot test.
According to the Agency, the United States Centers for Disease Control and Prevention and the European Centre for Disease Prevention and Control, use of the two-tiered method is based on credible scientific evidence.
Notes on serologic tests
- Serologic tests are insensitive during the first few weeks of infection. During this stage, patients presenting with Lyme disease symptoms should be diagnosed clinically. Testing of acute (first samples collected) and convalescent (collected 2-4 weeks later) blood samples may be helpful to confirm infection in some cases.
- The physician should specify, on the requisition, the possible exposure area (i.e. whether in North America or in Europe) as the tests done by the public health laboratories will vary, as the species of Borrelia can differ between continents and countries.
- In persons with illness > 1 month, only IgG testing should be performed (not IgM). A positive IgM test alone is not sufficient to diagnose current disease in these patients.
- Due to antibody persistence, a positive serologic test result cannot distinguish between active and past infection.
- Serologic tests cannot be used to measure treatment response (i.e. they should not be done as a “test of cure”).
- The enzyme immunoassay (EIA) test has low specificity and may yield false-positive results when used as a stand-alone test. EIAs may cross-react with antibodies to commensal or pathogenic spirochetes, some viral infections (e.g., varicella, Epstein-Barr virus), or certain autoimmune diseases (e.g., lupus).
Canadian laboratory diagnostic guidelines
Canadian laboratory diagnostic guidelines for Lyme disease are consistent with those followed by public health authorities in the United States and Europe and meet current international standards.
Public health professionals in these countries have concerns regarding reports from laboratories that may not be using properly validated tests or recommended standards for interpreting test results (CDC, MMWR, 2005). Further research is required to enhance current knowledge on new Borrelia species, and strains of other tick-borne pathogens to inform development of diagnostic methods that can reliably identify emerging pathogens.
Treatment
Treatment regimens listed in the following table are for localized (early) Lyme disease. Treatment guidelines for patients with disseminated (early and late) Lyme disease are outlined in the reference below (Wormser, et al., 2006).
These regimens are guidelines only and may need to be adjusted depending on a patient’s age, medical history, underlying health conditions, pregnancy status or allergies. Consult an infectious disease specialist, as needed for the most current treatment guidelines or for individual patient treatment decisions.
| Age Category | Drug | Dosage | Maximum | Duration in Days(Range) |
|---|---|---|---|---|
| Adults | Doxycycline | 100 mg, p.o., q 12 h. | N/A | 14 (14-21) |
| Cefuroxime axetil | 500 mg, p.o., q 12 h | N/A | 14 (14-21) | |
| Amoxicillin | 500 mg, p.o., q 8 h | N/A | 14 (14-21) | |
| Children | Amoxicillin | 50 mg/kg per day p.o., divided in 3 doses | 500 mg per dose | 14 (14-21) |
| Doxycycline* | 4 mg/kg per day p.o., divided into 2 doses | 100 mg per dose | 14 (14-21) | |
| Cefuroxime axetil | 30 mg/kg per day p.o., divided into 2 doses | 500 mg per dose | 14 (14-21) |
Note:
- For patients intolerant of amoxicillin, doxycycline, and cefuroxime axetil, the macrolides azithromycin, clarithromycin, or erythromycin, may be used, although they have lower efficacy. Patients treated with macrolides should be closely observed to ensure resolution of clinical manifestations.
- *Doxycycline is contraindicated in children younger than 8 years of age and in pregnant or lactating women. Amoxicillin is the drug of choice for these groups.
Although timely treatment with a recommended 14-21 day antibiotic course (or 28 day course for some types of disseminated Lyme disease) is effective to treat Lyme disease in most cases, some Lyme disease patients have persistent symptoms following treatment. Research continues into the causes of these persistent symptoms and methods of treatment. There is no evidence that persistent symptoms represent ongoing infection. Post-infectious inflammation, due to damage from the infectious process, will respond to anti-inflammatory drugs.
Lyme disease in pregnancy
A few early case reports of pregnant women with untreated Lyme disease described adverse outcomes, with babies stillborn or dying within 48 hours of birth, but no set pattern of abnormality was found. Subsequent large population studies showed no increased risks of adverse outcomes of pregnancies in women with Lyme disease who received appropriate treatment. A comparison of pregnancy outcomes, in areas where Lyme disease was highly endemic as well as non-endemic areas, showed no excess of adverse outcomes in the highly endemic areas (O’Connell, 2011).
Post-exposure antibiotic therapy
Some experts recommend that doxycycline be offered as a single dose of 200 mg (or 4.4 mg/kg for people weighing less than 45 kg, to a maximum dose of 200 mg) for people ≥ 8 years of age who have been bitten in an area with hyper endemic infection. Prophylaxis can be started within 72 hours after removal of a feeding blacklegged tick, even if it's been attached for ≥ 36 hours. There is no data on the use of amoxicillin as an alternate prophylactic antibiotic in younger children.
In Canada, such prophylaxis should be considered if the prevalence of B. burgdorferi in ticks is high. The Public Health Agency of Canada continues to monitor the evolving geographic distribution and prevalence of infected ticks and cases of Lyme disease.
Prevention
There is currently no vaccine available for Lyme disease. The best way to avoid Lyme disease is to protect against tick bites. Health professionals should advise their patients to take the following measures:
- Cover up if you think you might be entering an area where you may be exposed to ticks. Wear closed-toe shoes, long-sleeved shirts and pants. Pulling your socks over your pant legs prevents ticks crawling up your legs. Light-coloured clothing makes spotting ticks easier.
- Use insect repellents that contain DEET
 (concentration between 20-30%) or Icaridin. Repellents can be applied to clothing as well as exposed skin. Always read and follow label directions.
(concentration between 20-30%) or Icaridin. Repellents can be applied to clothing as well as exposed skin. Always read and follow label directions. - Shower or bathe within two hours of being outdoors to wash off unattached ticks. Daily “full body” checks for ticks should be performed. As nymphal ticks are the size of poppy seeds they are very difficult to detect. Ticks attach themselves to the skin and should be removed within 24-36 hours, which usually prevents infection. Be sure to check children and pets for ticks as well.
Surveillance of Lyme disease cases
Cases of Lyme disease in Canadians
Since December 2009, Lyme disease has been a nationally notifiable disease in Canada. This means that all cases that fit the surveillance case definition criteria should be notified by healthcare professionals to the local medical officer of health. The current case definitions for confirmed and probable classifications are:
Confirmed cases
- Clinical evidence of illness with laboratory confirmation by isolation of Borrelia burgdorferi from an appropriate clinical specimen, or by detection of B. burgdorferi deoxyribonucleic acid (DNA) by Polymerase Chain Reaction (PCR); or
- Clinical evidence of illness with a history of residence in, or visit to, an endemic area and with laboratory evidence of infection by approved serological methods and test interpretations.
Probable cases
- Clinical evidence of illness without a history of residence in, or visit to, an endemic area and with laboratory evidence of infection (i.e., positive or equivocal ELISA and positive IgM and/IgG western blots); or
- Clinician-observed EM without laboratory evidence but with history of residence in, or visit to, an endemic area.
The Agency currently has data for Lyme disease cases reported between 2009 and 2013*:
- 2009: 144 cases
- 2010: 143 cases
- 2011: 266 cases
- 2012: 338 cases
- 2013: 682 cases
- 2014: The Agency is still validating reports from provinces and territories. The final figure will be confirmed and reflected here.
Footnote *
These numbers may change slightly as provincial or territorial public health organizations can from time to time retroactively identify cases and update their statistics.
Although the Agency conducts surveillance both on ticks carrying the bacteria that cause Lyme disease and on human cases of Lyme disease, surveillance detects only a portion of the Lyme disease cases in Canada. The true number of Lyme disease infections in Canada is likely greater.
This is also true in the United States (US). Each year, approximately 30,000 cases of Lyme disease are reported by the Centers for Disease Control and Prevention (CDC); however this number does not reflect every case of Lyme disease. The CDC estimates that approximately 300,000 people are diagnosed with Lyme disease each year in the US. For additional information, please visit the CDC’s website![]() .
.
The Agency relies on the provinces and territories to report the number of Lyme disease cases occurring in their jurisdictions on an annual basis. In order to most accurately reflect the occurrence of Lyme disease cases in Canada each year, healthcare professionals need to remain vigilant in diagnosing Lyme disease and promptly reporting cases to their public health regional authorities.
Surveillance for Lyme disease risk in our environment
The Agency works with provincial and territorial public health organizations, health authorities and other experts to undertake surveillance to identify where risk of acquiring Lyme disease occurs in Canada.
This is because:
- For public health professionals, knowledge of where risk from Lyme disease occurs can help targeting of awareness-raising information on preventive and control methods to the people who may be particularly at risk from Lyme disease, due to their geographic location and/or occupation (e.g. forester, park worker) or choice of leisure activity (camping, golfing, etc.).
- For health care professionals, knowledge of a patient’s exposure to known or possible emerging Lyme disease risk areas (Table 1, Fig 1 and Fig 2) is an important parameter for Lyme disease diagnosis.
- Knowledge of where known endemic areas occur (Table 1 and Fig 1) is important when reporting Lyme disease cases by public health and health care professionals in our national surveillance system, as consideration of exposure of cases to endemic areas determines classification of cases as “confirmed” or “probable”.
Two complementary methods of surveillance are used:
‘Passive’ surveillance involves the voluntary submission of ticks found on humans and domestic animals, by veterinarians and healthcare professionals (Ogden et al., 2006; 2010). This method can raise the suspicion of areas where ticks are establishing.
‘Active’ field surveillance involves collection of ticks and/or wild animal hosts by standardised methods to determine whether populations of vector ticks and endemic cycles of Borrelia burgdorferi transmission have become established. These methods are used to identify where tick populations are becoming established (Lyme disease risk areas), and, when multiple visits to the same site are possible, to confirm the occurrence of a Lyme disease endemic area (Health Canada 1991).
Where risk of acquiring Lyme disease occurs in Canada?
The risk of Lyme disease occurs where ticks that carry the Lyme disease-causing agent B. burgdorferi are found.
In Canada, the blacklegged tick (Ixodes scapularis, which is becoming established from Manitoba eastwards) and the western blacklegged tick (Ixodes pacificus, which occurs in British Columbia) are the species that transmit B. burgdorferi. These ticks can also carry other less common infectious agents. Other tick species are known to transmit the bacterium that causes Lyme disease in nature, but these ticks live in the nests and burrows of their wild animal hosts and rarely bite humans.
The greatest risk of Lyme disease in Canada occurs where populations of the ticks are established because in these locations, ticks are most abundant. These locations are termed ‘Lyme endemic areas’ when their presence is confirmed by multiple years of active field surveillance, and ‘suspect endemic areas’ when only one year of active field surveillance has been undertaken. However, surveillance shows that the ticks have become established over a much wider area (termed Lyme disease risk areas) than that of the more highly studied endemic areas (Ogden et al. 2014a, b).
These areas are defined as:
A confirmed Lyme disease endemic area is defined as a locality where active field surveillance has detected i) reproducing populations of the tick vector as confirmed by the presence of all three stages (larva, nymph and adult) on resident animals or in the environment for at least 2 consecutive years; and ii) the agent of Lyme disease (B. burgdorferi) has been detected in ticks and/or wild animal hosts collected from the locality by culture, molecular methods (specific PCR), or immunofluorescent antibody staining (IFA) (Health Canada 1991).
A suspected Lyme disease endemic area is a locality where active field surveillance has revealed the presence of multiple ticks at one or more visits, suggesting that the tick vector is becoming established, and where B. burgdorferi has been detected in ticks or animals collected from the site.
A Lyme disease risk area is a locality or region where tick vectors of Lyme disease have been detected by active field surveillance, whether or not B. burgdorferi has been detected in tick or animal samples (Ogden et al. 2014a).
The geographic extent and degree of risk in endemic and risk areas in Canada varies from one location to another and is changing over time.
Surveillance conducted in recent years indicates that established populations of blacklegged ticks are spreading their geographic scope, and are increasing in number, in eastern and central Canada. In contrast, in British Columbia there is little evidence for expansion of tick populations and according to the British Columbia Ministry of Health, surveillance conducted over the past decade has shown a plateau in the numbers of infected tick populations, which is different to the spread seen in other parts of Canada.
The potential expansion of localized tick populations makes it difficult to precisely define the geographic limits of any given population; however people living or visiting areas adjacent to established tick populations may have a greater chance of contact with blacklegged ticks.
The proportion of ticks in a geographic area that are infected with the bacterium causing Lyme disease (the prevalence of infection) varies geographically and over time. This is particularly marked in the differences between areas in British Columbia and in central and eastern Canada. In British Columbia and in adjacent Pacific northwestern states, the proportion of I. pacificus ticks that are infected with the Lyme disease agent is usually much lower (<1%) than the proportion of I. scapularis ticks that are infected in endemic areas in northeastern US and central and eastern Canada (between 10 and 60% of ticks). This is partly because of differences in the types of hosts that the different tick species feed upon. The proportion of infected I. scapularis ticks is often greater where tick populations have been established for long periods of time (such as Long Point), compared to areas with newly established tick populations. Based on surveillance data, as many as 60% of the adult I. scapularis ticks at Long Point are infected; however, infection rates in adult I. scapularis ticks are more often between 10 and 25% at the other localities where ticks are established.
Medical and public health professionals should be aware that there is a low risk of Lyme disease being contracted almost anywhere in Canada because migratory birds transport infected ticks over large geographic distances. Nevertheless the risk of coming in contact with infected blacklegged ticks is much higher in areas where tick populations are established because these areas are where the numbers of ticks is greatest and where nymphal ticks are found. The proportion of infected ticks is typically higher in adult ticks compared to nymphs stages (larvae are not infected). However, people are most likely to acquire Lyme disease from a nymph because this stage is more numerous than adult ticks and nymphs are active in spring and summer when people are more likely to be out in the woodlands where the ticks occur. Nymphs are also very small (see Figure 4), and thus more likely to go unnoticed, allowing it to feed for a sufficient amount of time for the Lyme disease bacterium to be transmitted (over 36 hours).
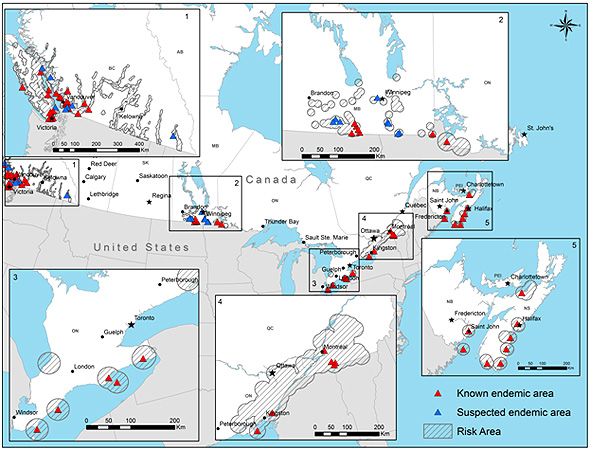
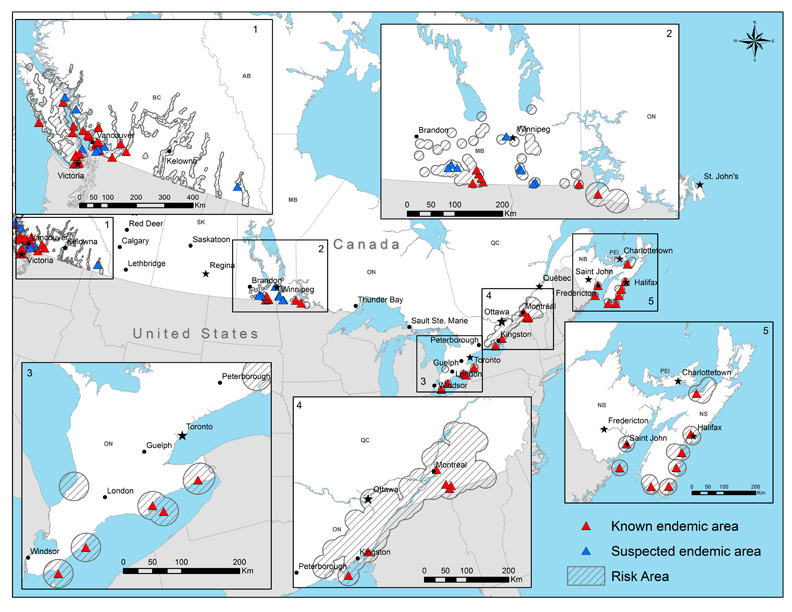
Our current knowledge of the occurrence of Lyme disease endemic and risk areas, based on active surveillance in the field, is detailed in Table 1 and Figure 1.
| Province* | Locations of endemic and risk areas |
|---|---|
| *To date no evidence of endemic or risk areas for Lyme disease has been found in Alberta, Saskatchewan, Prince Edward Island, Newfoundland & Labrador or the Territories. | |
| British Columbia | Known and suspect endemic Lyme disease areas are Vancouver Island, particularly along the eastern coast, and the Vancouver Lower Mainland. Possible risk areas include the southwestern mainland coastal region (Sunshine Coast) and the southern interior valley regions of the province. It should be noted that trends in prevalence and spread of Lyme disease in British Columbia differ from the rest of Canada. The British Columbia Ministry of Health has regularly surveilled risk areas over the past decade, and has reported a plateau in the numbers of infected tick populations compared to the spread seen in other parts of Canada. Partly because of differences in the types of hosts that they feed upon, the proportion of I. pacificus ticks that are infected with the Lyme disease agent is usually much lower (<1%) than the proportion of I. scapularis ticks that are infected. |
| Manitoba | There are six regions where known or suspect endemic areas occur: an area of the west side of Lake of the Woods (known endemic), the area of the Pembina escarpment including Pembina Valley Provincial Park (known endemic), the region of St. Malo (suspect area), the Vita/Arbakka region including the Roseau river (suspect area), Beaudry Provincial Park and the Assiniboine River (suspect area), locations adjacent to the Agassiz and Sandilands provincial forests (suspect area). Risk areas include locations in southern Manitoba along the border with the US from south of Brandon to Lake of the Woods, and around Winnipeg. |
| Ontario | There are seven known endemic areas: Pointe-Pelee National Park, Rondeau Provincial Park, Turkey Point Provincial Park, Long Point peninsula including Long Point Provincial Park and the National Wildlife area, Wainfleet bog near Welland on the Niagara peninsula, Prince Edward Point and parts of the Thousand Islands National Park. Risk areas are locations around Kingston and along the Saint Lawrence valley to the border with Quebec that extend north east towards Ottawa. Risk areas have also been identified in western Ontario in the region of Lake of the Woods and at Pinery Park on the shore of Lake Huron. |
| Quebec | There are five known endemic areas in Montérégie, in the south of Québec. Risk areas cover much of Montérégie, extending to parts of Estrie and Centre du Québec. |
| New Brunswick | There are two known endemic areas in New Brunswick in the Millidgeville area of Saint John and North Head, Grand Manan Island. |
| Nova Scotia | There are six known endemic areas in Nova Scotia in the areas of Halifax Regional Municipality and in areas of the counties of Lunenburg, Shelburne, Yarmouth, Pictou and Queens. Locations around known endemic areas are possible risk areas. |
Figure 1 shows the locations where the current risk from tick bites and Lyme disease is known to occur. Locations where ticks and Lyme disease risk are known are called ‘endemic areas’ (‘known’ endemic areas if ticks and Lyme disease risk have been confirmed over several years of field study or by the occurrence of multiple human cases, otherwise they are called ‘suspect’ endemic areas). Also shown are Lyme disease risk areas (the hatched areas) where surveillance and research studies (risk mapping in BC(PDF Document)![]() ) suggest ticks and possible Lyme disease risk have begun to become established.
) suggest ticks and possible Lyme disease risk have begun to become established.
{kind=link}
Field surveillance for ticks cannot cover the whole of Canada because of the immensity of our country, and because of the practical difficulties in performing surveillance in remote areas and on privately held land. But, tick populations are expanding across the country and as such, Lyme disease can be acquired outside the currently identified areas. The Agency is enhancing its Lyme disease surveillance to better predict new and emerging areas of risk. In collaboration with provincial, public and animal health organizations, and with Canadian universities, the Agency developed a map (Figure 2) to show areas predicted to be at risk of becoming Lyme disease endemic. The objectives of this map are to help guide surveillance and preventative efforts and to provide a resource for those working and participating in leisure activities outdoors. The map is constructed using the Agency’s current knowledge of the biology of the blacklegged tick and of the environmental factors that limit its survival (Ogden et al., 2008), and has performed well in field validation to date (Ogden et al., 2008; 2010).
Please click here to view the British Columbia Centre for Disease Control's website (Available in English only)![]() on Lyme disease. A risk map for the occurrence of Lyme endemic areas in British Columbia can be found on their page.
on Lyme disease. A risk map for the occurrence of Lyme endemic areas in British Columbia can be found on their page.
Figure 2 shows areas predicted to be at risk for emergence of Lyme endemic areas in eastern and central Canada in the coming decade.
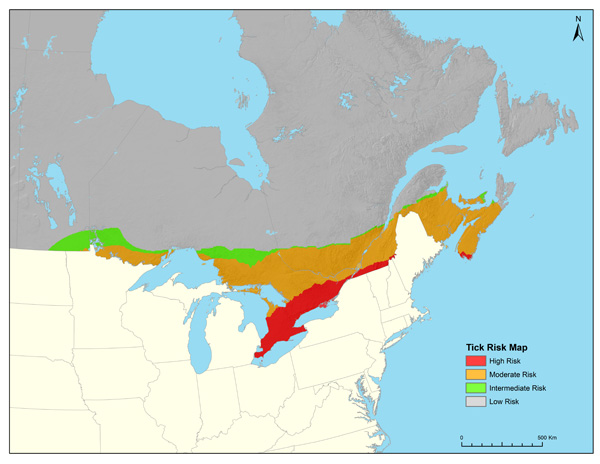
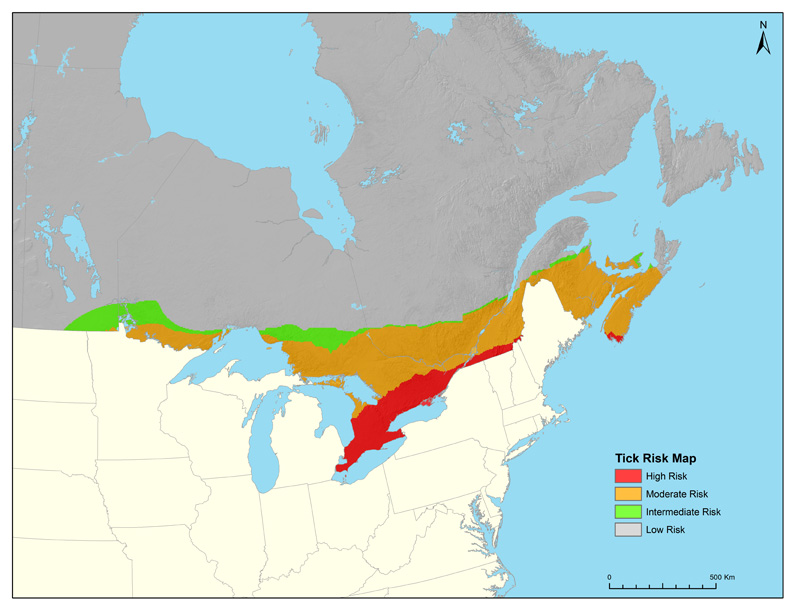{kind=link}
The coloured zones on the map indicate current predictions for regions where Lyme endemic areas are most likely to emerge in central and eastern Canada in the coming decade, provided that suitable woodland habitat for the blacklegged tick exists. The orange zone indicates the main extent of locations where Lyme endemic areas may emerge. The red zones indicates areas with the highest risk for emergence of new Lyme endemic areas, while in the green area the risk is predicted to be low. The grey zone indicates areas where, in general, the risk of Lyme endemic area emergence is predicted to be very low and risk of Lyme disease is mostly restricted to that posed by ‘adventitious’ ticks dispersed by migratory birds from Lyme endemic areas in Canada and the US. Even so, in some localized areas of the grey risk zone, local environmental conditions may be suitable for Lyme endemic areas to emerge.
Risk of acquiring Lyme disease during travel out of Canada
Visitors to the United States (US) should note that there are extensive areas with established blacklegged tick populations, particularly in the northeast and upper Midwest regions. More information on Lyme in the US can be found on the Centers for Disease Control and Prevention web site![]() . Lyme disease also occurs in Europe and some parts of Asia
. Lyme disease also occurs in Europe and some parts of Asia![]() .
.
Other tick-borne diseases in Canada
Both the blacklegged tick and western blacklegged tick can transmit pathogens other than the agent of Lyme disease. These pathogens are all zoonoses (i.e. infections of animals that can cause disease in humans) for which the natural hosts are wild animals. Of importance are the bacterium Anaplasma phagocytophilum, which causes Human Granulocytic Anaplasmosis (HGA: Wormser et al., 2006), the protozoal parasite Babesia microti, which causes human babesiosis, and Powassan encephalitis virus (POWV) including the deer tick virus lineage, both of which can cause encephalitis. Other bacteria carried by these ticks include Borrelia bissettii, B. carolinensis and B. kurtenbachii although whether these bacteria cause disease in humans in North America is unknown. The bacterium B. miyamotoi occurs at low prevalence in blacklegged ticks and, recently, human cases (mostly suffering influenza-like illnesses) associated with B. miyamotoi have been discovered in the United States. Vigilance by physicians for cases associated with this bacterium is recommended (Dibernardo et al 2014).
Tick-borne diseases transmitted by other tick species also occur in Canada and include Rocky Mountain Spotted Fever (caused by Rickettsia rickettsii), transmitted primarily by the Rocky Mountain wood tick (Dermacentor andersoni) and tularaemia (caused by the bacterium Francisella tularensis), transmitted by the American dog tick (Dermacentor variabilis Figure 3). Powassan encephalitis is caused by Powassan virus (POWV), transmitted by Ixodes cookei ticks and relapsing fever (caused by the bacterium Borrelia hermsii) is transmitted by soft bodied (Argasid) ticks in southern British Columbia. Tick-borne diseases carried by the ‘Lone Star tick’ Amblyomma americanum, which include Human Monocytic Ehrlichiosis caused by the bacterium Ehrlichia chaffeensis, could also occur in Canada, but are rare. These diseases are associated with ticks dispersed from the US by migratory birds.
A toxin in the saliva of adult female Rocky Mountain wood ticks (RMWT) can cause paralysis in humans and animals, on which these ticks feed. Paralysis ascends beginning in the legs and spreads to other muscles during the period the tick is feeding. Paralysis can extend to muscles important for respiration, and if not diagnosed and treated early, the paralysis can result in death. Simple removal of the feeding ticks is usually sufficient for recovery (Gregson, 1973). Rocky Mountain wood ticks are found from central Saskatchewan to British Columbia, although RMWT in the Canadian prairies may be genetically incapable of causing paralysis (Lysyk, 2010). Other tick species endemic to Canada, such as American dog ticks and blacklegged ticks, have been linked to cases of tick paralysis, but not in Canada (Gregson 1973).
Identifying blacklegged ticks
Blacklegged ticks are considerably smaller than the more common American dog tick (often called the wood tick), Dermacentor variabilis. Adults of the blacklegged ticks lack the white marking seen on the dorsum of adult dog ticks (Figure 3). Before feeding, blacklegged adult females are approximately 3-5 mm in length and red and dark brown in colour. The pre-adult stages (larvae and nymph) are much smaller and lighter in colour (Figure 4). All stages except adult males increase in size and change colour as they feed upon a host. For example, it is not uncommon for adult females to reach the size of a small grape and they typically go through a change in colour from whitish as they start feeding to dark gray to nearly black when fully fed (Figure 5). Larvae and nymphs also increase proportionally in size and go through a similar change in colour (Figure 6).
Figure 3: Unfed adult blacklegged ticks (top row) and adult American dog (wood) ticks (bottom row). Note the difference in colour patterns and relative size.

Figure 4: Unfed life stages of the blacklegged tick (1-larva, 2-nymph, 3-adult male, 4-adult female). Sizes presented in relation to underlying 10-cent coin.

Figure 5: Female blacklegged ticks in various stages of feeding. Note the change in size and colour.

Figure 6: Unfed, partially fed and fully engorged nymphs of the blacklegged tick. Note the change in size and colour.

Removing Ticks
To remove ticks that are embedded in skin, use tweezers to carefully grasp the tick as close to the skin as possible and pull slowly upward, avoiding twisting or crushing the tick. If members of the public are concerned about removing a tick from themselves or a member of their family, the Agency recommends that they ask for assistance from a healthcare professional who can also advise on possible symptoms of tick-borne diseases to permit early recognition of infection and prompt treatment. In messaging to the general public, the Agency has advised that patients keep any ticks they remove themselves in an airtight bag or pill vial and note the location and date of the bite. They are then advised to watch for symptoms, and to see their healthcare professional immediately, should symptoms appear. Note: the Agency recommends patients take the tick with them to their medical appointment, to support healthcare professionals in their clinical assessment of potential causes for the onset of illness.
Submitting ticks for identification and testing
When possible, ticks should be sent to provincial collaborators who will identify the tick and then forward only the blacklegged ticks to the Agency's National Microbiology Laboratory (NML). Staff at the NML will conduct testing for the Lyme disease agent as well as several other disease-causing agents. It should be remembered that this tick testing program is designed specifically for surveillance to gain a better understanding of the distribution of blacklegged ticks and their associated pathogens. Tick testing has very limited practical use for clinical diagnostic purposes (i.e., to determine whether to treat or not) and there are established guidelines for prophylactic treatment of patients with documented exposure to blacklegged ticks (Wormser et al. 2006). For information on where to send tick specimens in your area, contact the NML through phone or email at:
National Microbiology Laboratory
Phone: (204) 789-2000
Email: ticks@phac-aspc.gc.ca
Please note that it usually takes at least two weeks for ticks submitted to the NML to be identified, tested, and for results to be reported to the original submitter. During the peak periods of adult activity (October to December), the processing time at the NML can extend to 4-6 weeks because of the large volume of tick samples received.
Download PDF document:
Please follow the guidelines for handling and shipping ticks and complete and attach a Tick Submission Form (PDF Document - 766 KB - 1 page) with the submission.
References:
Bacon RM, Kugeler KJ, Mead PS Surveillance for Lyme disease--United States, 1992-2006. MMWR Surveill Summ. 2008 Oct 3;57(10):1-9.
Bockenstedt, L. K. (2008). Infectious Disorders: Lyme Disease. In J. H. Klippel, J. H. Stone, L. J. Crofford, & P. H. White, Primer on the Rheumatic Diseases (13th ed., pp. 282-289). New York: Springer.
Centers for Disease Control and Prevention. (2005, February 11). Caution regarding testing for Lyme disease. MMWR, 54(5), 125.
Centers for Disease Control and Prevention. (2011, February 5). http://www.cdc.gov/ncidod/dvbid/lyme/index.htm.
Centers for Disease Control and Prevention. (2013, December 13). Three Sudden Cardiac Deaths Associatied with Lyme Carditis - United States, November 2012 - July 2013. MMWR, 62(49), pp. 993-996.
Dibernardo, A., Cote, T., Ogden, N. H., Lindsay, LR. (2014). The prevalence of Borrelia miyamotoi infection, and co-infections with other Borrelia spp. In Ixodes scapularis ticks collected in Canada. Parasites & Vectors. In Press.
Feder, H., Johnson, B., & O'Connell, S. e. (2007). A critical appraisal of 'chronic Lyme disease'. N. Engl. J. Med., 357, pp. 1422-1430.
Hatchette, T.F., Davis, I, & Johnston, B.L. (2014, May 29). Lyme disease: clinical diagnosis and treatment. CCDR, Vol 40-11, pp. 194-208.
Lindsay, L.R., Bernat, K. & Dibernardo, A. (2014, May 29). Laboratory diagnostics for Lyme disease. CCDR, Vol 40-11, pp. 209-217
Marques, A. R. (2010). Lyme Disease: A Review. Curr Allergy Asthma Rep, 10, pp. 13-20.
Meyerhoff, J. O., & Diamond, H. S. (2014, September 10). Medscape. Consulted September 18, 2014, on Medscape Reference: Drugs, Diseases & Procedures: http://emedicine.medscape.com/article/330178-clinical
O'Connell, S. (2011). Lyme borreliosis. In S. Palmer, L. Soulsby, P. Torgerson, & D. W. Brown, Oxford Textbook of Zoonoses: Biology, Clinical Practice, and Public Health Control (2nd ed., pp. 82-91). Oxford: Oxford University Press.
Ogden, N. H., St-Onge, L., Barker, I. K., Brazeau, S., Bigras-Poulin, M., Charron, D. F., . . . O'Callaghan, C. (2008, May 22). Risk Maps for range expansion of the Lyme disease vector, Ixodes scapularis, in Canada now and with climate change. International Journal of Health Geographics, 7(24), 1-15.
Ogden, N., Artsob, H., Lindsay, L., & Sockett, P. (2008, October). Lyme Disease: A zoonotic disease of increasing importance to Canadians. Canadian Family Physician, 54, 1381-1384.
Ogden, N., Lindsay, L., Morshed, M., Sockett, P., & Artsob, H. (2008). The rising challenge of Lyme borreliosis in Canada. Canadian Communicable Disease Report, 34, 1-19.
Ogden NH, Koffi JK, Lindsay LR (2014a) Assessment of a screening test to identify Lyme disease risk. Canada Communicable Disease Report. 40, 83-87
Ogden NH, Koffi, JK, Pelcat Y, Lindsay LR (2014b) Environmental risk from Lyme disease in central and eastern Canada: a summary of recent surveillance information. Canada Communicable Disease Report. 40, 74-82
Stonehouse, A., Studdiford, J. S., & Henry, C. A. (2007). An update on the diagnosis and treatment of early Lyme disease: "Focusing on the Bull's Eye, you may miss the mark". The Journal of Emergency Medicine, 39(5), e147-e151.
U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. (2013 1st Edition). Tickborne Diseases of the United States. Fort Collins CO: Centers for Disease Control and Prevention.
Wormser, G., Dattwyler, R., Shapiro, E., & al., e. (2006). The clinical assessment, treatment and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases of America. Clin Infect Dis, 43, 1089-1134.
To share this page just click on the social network icon of your choice.